Most advice on selling to pharmaceutical companies is too generic to be useful. It treats pharma like any other enterprise vertical with a few compliance wrinkles. That's a mistake.
Pharma buyers don't respond to broad claims, vague transformation language, or recycled SaaS messaging. They work inside a system shaped by clinical evidence, regulatory milestones, launch planning, market access constraints, and internal politics that cut across scientific, commercial, legal, procurement, and IT teams. If your outreach sounds like it could have gone to a retail brand or a software company, it won't land.
The buyer is also less stable than many sellers assume. Recent reporting points to a meaningful shift toward a more fragmented ecosystem shaped by direct-to-patient, employer, and transparent-price models. Manufacturers are experimenting with direct-to-consumer and direct-to-employer pathways, which changes who the buyer is. In some situations, you're no longer selling only into a pharma company. You're selling into a network that can include employers, health plans, PBMs, specialty pharmacies, and sometimes patients themselves, as covered in Managed Healthcare Executive's reporting on more direct ways of selling and buying prescription products.
That shift makes lazy vertical messaging even more dangerous. The old playbook assumed one commercial team, one procurement path, one budget owner. That's not reliable anymore. You need a point of view on channel strategy, access friction, launch risk, and stakeholder alignment before you ask for time.
Why Generic Sales Tactics Fail in Pharma

A lot of reps think good discovery can make up for limited domain knowledge. In pharma, it usually can't. The buyer often knows the science, the process, and the operational constraints far better than the seller. If you show up with a generic deck and hope to “learn their business” live on the call, they'll spot it immediately.
That's because pharma teams don't buy in a vacuum. A clinical leader evaluates risk differently from a commercial leader. A market access stakeholder cares about evidence that supports adoption and reimbursement. IT looks for integration, data handling, security, and validation. Procurement still wants bargaining power, but it rarely drives the full decision on its own.
Why domain fluency matters
Selling to pharmaceutical companies requires domain fluency. Credibility comes from knowing their pipeline, not just your pitch. You should know what assets matter, where the company is investing, what therapeutic areas it's expanding into, and what operational pressure the team is likely under.
That doesn't mean pretending to be a scientist. It means speaking with enough precision that a scientific or medical stakeholder doesn't dismiss you in the first minute.
A weak opening sounds like this:
- Generic value claim: “We help pharma companies streamline commercial execution and improve visibility.”
- No situational context: “Would love to show how we support growth.”
- Zero proof of homework: Nothing about pipeline stage, launch readiness, market access hurdles, or internal change.
A credible opening sounds different:
- Specific business context: “You've got a program moving closer to a commercial inflection point, and that usually forces tighter coordination between commercial, medical, and access teams.”
- Relevant problem framing: “At that point, these teams aren't short on dashboards. They're short on aligned evidence and stakeholder readiness.”
- Useful reason to talk: “If that's the case, it may be worth comparing where launch planning is getting blocked.”
Practical rule: If your first message could work unchanged for fintech, manufacturing, and pharma, it's not a pharma message.
What fails most often
The biggest mistake isn't being too simple. It's being too abstract.
Pharma buyers will challenge specifics. They'll ask what data you need, how your process handles review, where your system fits in regulated workflows, and what internal team gets value first. If you can't answer cleanly, the call ends politely and goes nowhere.
Three patterns fail over and over:
-
Product-first messaging
Leading with features before proving you understand the buyer's operating context. -
Shallow personalization
Referencing a press release without connecting it to a real commercial or operational consequence. -
ROI-only positioning
Leaning on generic efficiency language when the primary issue is evidence, access, readiness, or risk reduction.
Relationship quality still matters in pharma. It matters a lot. But timing and relevance matter too. A trusted rep with bad timing gets ignored. A well-timed rep with no credibility gets screened out. The win comes from combining both.
See Salesmotion in action
Take a self-guided interactive tour — no signup required.
Mapping the Complex Pharma Buying Committee
Pharma deals rarely stall because one person says no. They stall because five people have different definitions of acceptable risk, acceptable evidence, and acceptable disruption.
That changes how you build the account plan. A standard enterprise playbook assumes you can find a champion, prove ROI, and let that person pull the deal through. In pharma, that usually breaks down. The buyer group is broader, the scrutiny is higher, and a stakeholder you never met can slow the deal late because your process does not fit a regulated workflow.
Start with decision roles, not job titles
Titles in pharma are inconsistent. Decision roles are not.
A commercial operations lead at one company may play the same role as a business excellence director or franchise VP at another. If you map by title alone, you miss the people who ultimately shape the outcome. If you map by role in the decision, the picture gets clearer.
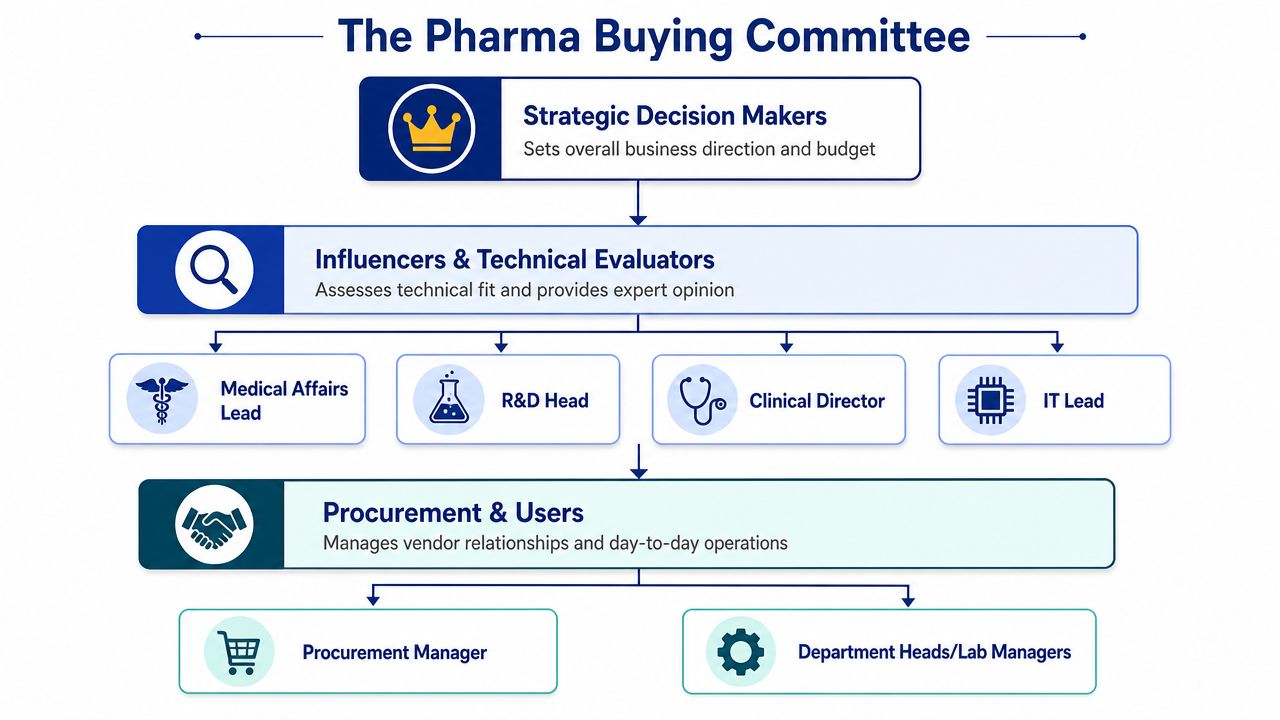
Build the account around four groups:
-
Economic buyer
The person who can approve budget or justify why this project should get funded now. In pharma, that often sits in commercial operations, digital, analytics, market access leadership, or a business unit role. -
Technical evaluator
The person who tests whether your product can survive internal review. This often includes IT, information security, data governance, validation, privacy, or an operations leader who understands the process well enough to spot implementation risk. -
Workflow owner
The team that will live with the change after signature. In pharma, this matters more than many reps expect. If your solution adds review steps, creates training overhead, or interrupts established handoffs between commercial, medical, and access teams, resistance shows up late and kills momentum. -
Internal champion
The person who feels the pain, sees the use case, and helps you get meetings. That matters. It is still only one part of the deal.
If your team needs a repeatable way to build that map, use this framework for how to find decision-makers in a company.
What each stakeholder is really evaluating
Pharma buying committees do not evaluate one thing. They evaluate different risks at the same time.
Commercial leaders tend to ask whether this helps the business make better decisions around launch, field execution, access, or performance tracking. Scientific and clinical stakeholders ask whether the output is credible, defensible, and usable in practice. IT and data teams focus on integration, governance, support load, privacy, and security exposure. Procurement wants scope clarity, vendor risk clarity, and a process they can move forward without surprises.
That is why one generic deck performs poorly here. The same message that gets a first meeting with a commercial leader can create friction with medical, security, or procurement if it sounds too broad, too promotional, or too light on evidence.
A useful account map answers a harder question than "who is involved?" It answers "what would make each person comfortable enough to keep this moving?"
Bring risk owners in early
Late-stage surprises are expensive in pharma. The usual culprits are legal, procurement, security, privacy, and quality.
I learned this the hard way. Deals that looked healthy at the user level often slowed once risk owners got involved and realized the seller had not prepared for validation requirements, data handling questions, or vendor review steps. By then, enthusiasm was no longer enough to carry the process.
Salesmotion's guidance on selling to life sciences makes the same point. In regulated buying environments, showing readiness on items such as SOC 2, GDPR, and GxP can reduce friction during procurement and review.
Do not dump a security packet into the first email. Do know, before the second serious conversation, how you will answer questions like these:
- Who owns the budget?
- Who can stop the deal on compliance, validation, security, or procurement grounds?
- Whose day-to-day workflow changes if this gets approved?
- Who gains enough business value to sponsor the project internally?
If those answers are still fuzzy, you do not have a mapped buying committee. You have early interest. In pharma, those are not the same thing.

“We're no longer fishing. We know who the right customers are, and we can qualify them quickly. Salesmotion has had a direct impact on pipeline quality.”
Andrew Giordano
VP of Global Commercial Operations, Analytic Partners
Decoding Critical Pharma Buying Signals
Most enterprise sellers mistime pharma outreach. They contact accounts when something has already been announced publicly and assume the window is open. Sometimes it is. Often it isn't. Pharma teams buy around moments of pressure, uncertainty, budget release, leadership change, and strategic transition.
That's why signal-based selling matters so much here. You need to know when the account has a real reason to evaluate something now.
The signals that change urgency
The strongest signals are the ones that force a company to revisit plans, headcount, systems, partners, or risk. In pharma, that often clusters around product development milestones, commercialization planning, and leadership changes.
A few that matter most in practice:
-
Clinical trial progress
When a program advances, the operational conversation usually changes with it. Teams start thinking differently about scale, evidence, launch planning, cross-functional coordination, and partner readiness. -
FDA milestone timing
Approval-related dates and regulatory milestones concentrate executive attention. Even before a final outcome, they can trigger budget decisions, internal projects, and new vendor reviews. -
Earnings call language
Listen for therapeutic area expansion, launch investment, commercial buildout, digital transformation language, or comments that suggest execution risk. Public commentary often tells you where leadership wants change. -
Leadership changes
A new executive can reset priorities faster than almost any other event. In the field, one of the strongest triggers is a new VP of Commercial Operations. New leaders often re-evaluate inherited vendors, inherited workflows, and inherited reporting structures.
Key pharma buying signals and their meaning
| Signal | Source | What It Means (The 'Why Now') |
|---|---|---|
| Clinical trial progression | Clinical trial databases, company updates | The company may be moving from research emphasis toward broader operational readiness and cross-functional planning. |
| FDA milestone or PDUFA timing | FDA-related disclosures, company communications | Leadership attention is concentrated. Teams may be preparing for launch, scenario planning, or post-decision execution. |
| New VP of Commercial Operations | Leadership announcements, LinkedIn, press releases | A new operator often reviews systems, partners, and process gaps quickly. This is one of the cleanest windows for vendor evaluation. |
| Therapeutic area expansion | Earnings calls, investor materials | Expansion usually creates new planning needs, new stakeholder groups, and pressure to adapt existing infrastructure. |
| Commercial hiring or team buildout | Job postings, org announcements | The company is investing in execution capacity. That often signals upcoming process redesign or tooling needs. |
For teams that want a more systematic approach, life sciences buying signals is a useful reference for monitoring the kinds of triggers that create timely outreach windows.
What timing really looks like
The mistake isn't just missing the signal. It's misunderstanding what the signal means.
A PDUFA date, for example, isn't merely “good timing.” It can indicate very different needs depending on the account. One team may be preparing for launch coordination. Another may be trying to de-risk access planning. Another may be heads-down on regulatory communication and not ready for a broad vendor conversation. The seller has to interpret the event, not just notice it.
The same goes for earnings calls. If leadership talks about a new therapeutic area, don't email saying, “Congrats on the expansion.” That's empty. Tie the signal to an execution problem. New area expansion often means new stakeholders, fresh evidence requirements, and uncertainty about what existing systems can support.
When pharma teams change strategy, they don't immediately buy software. They first try to understand what the change breaks.
That's the opening. Your outreach should connect the trigger to a pressure point they're likely dealing with right now.
Crafting a Credible, Evidence-Based Message
Most pharma messaging fails because it's written from the vendor's perspective. It starts with the product, then adds a few personalized lines, then asks for a meeting. That structure works poorly with buyers who expect you to understand the business problem before you introduce yourself.
The better approach is to build around commercial insight. Recent commercialization guidance emphasizes that manufacturers need to build the value story, map the patient journey, and segment payers and providers early. It also argues that messaging should focus on things like analogs, patient journey friction, payer restrictions, or distribution complexity rather than standard ROI claims, as discussed in Drug Channels' analysis of starting with the end in mind in pharma commercialization.
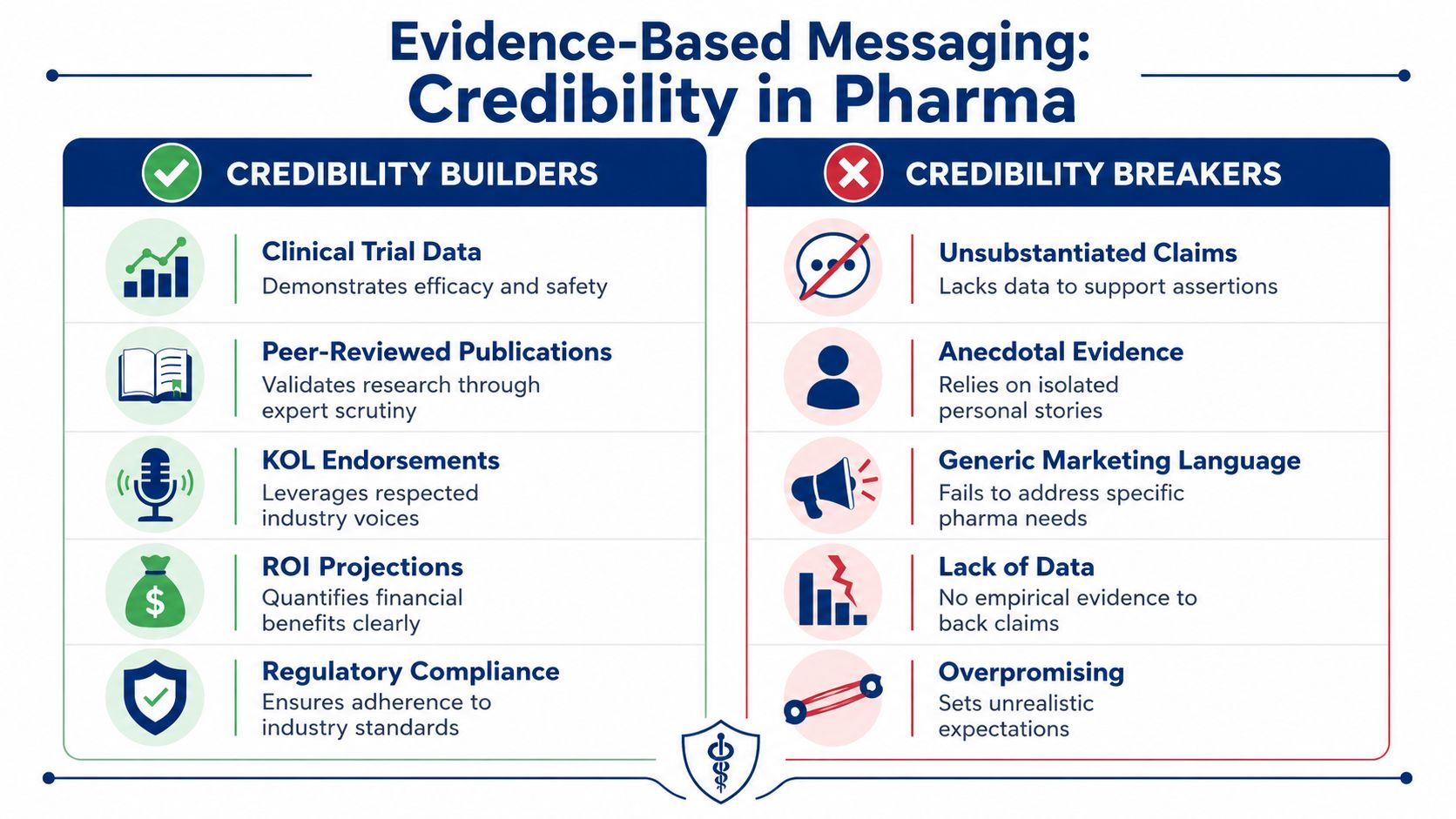
What credible messaging sounds like
A credible message to pharma does three things well.
First, it shows you understand the company's context. Not with trivia, but with business relevance.
Second, it frames a problem in language the buyer already uses internally. That may be launch readiness, patient journey friction, evidence gaps, access constraints, channel complexity, or cross-functional misalignment.
Third, it gives them a reason to engage now that isn't “book a demo.”
Here's a simple test. Ask whether your message answers this question:
What evidence, stakeholder map, and launch-risk context does this buyer need before they'll even take a meeting?
If it doesn't, rewrite it.
A practical do and don't breakdown
Don't write this:
- Weak opener: “We help pharmaceutical companies improve efficiency across commercial operations.”
- Weak claim: “Our platform delivers better visibility and stronger ROI.”
- Weak CTA: “Open to a quick intro next week?”
It's harmless, but it sounds like every other vendor.
Write this instead:
- Contextual opener: “You're likely coordinating more tightly across commercial, medical, and access as this program moves closer to a launch decision.”
- Problem frame: “That's usually where teams find that stakeholder alignment and usable evidence lag behind the plan.”
- Reason to talk: “If you're pressure-testing launch risk and internal readiness, I can share how other teams structure that early conversation.”
That kind of message respects the buyer's world. It doesn't overclaim. It also doesn't pretend you've solved anything before the first call.
Domain fluency beats enthusiasm
Pharma buyers don't need more enthusiasm. They need precision.
Use their language carefully. Mention the pipeline when relevant. Reference the therapeutic area only if you understand the implications. If market access is central, talk about payer restrictions or distribution complexity. If you're writing to clinical operations, center compliance, accuracy, and process fit. If you're writing to procurement, total cost of ownership and implementation risk matter more than visionary language.
A simple way to tighten your message is to use a structured customer value proposition template before you write outreach. It forces you to connect your offer to an actual business condition instead of defaulting to product slogans.
Generic pitches fail in pharma because they ask the buyer to do the interpretive work. Strong pitches do that work first.
“We have very limited bandwidth, but Salesmotion was up and running in days. The template made it easy to load our accounts and embedding it in Salesforce was simple. It was one of the easiest rollouts we've done.”
Andrew Giordano
VP of Global Commercial Operations, Analytic Partners
Executing a Multi-Threaded Sales Cadence
Once the account is mapped and the trigger is clear, execution becomes a coordination problem. It is here that much solid strategy falls apart. Reps know they should multi-thread, but what they do is send one decent email to one contact and wait.
That's not a cadence. That's hope.
What a real pharma cadence looks like
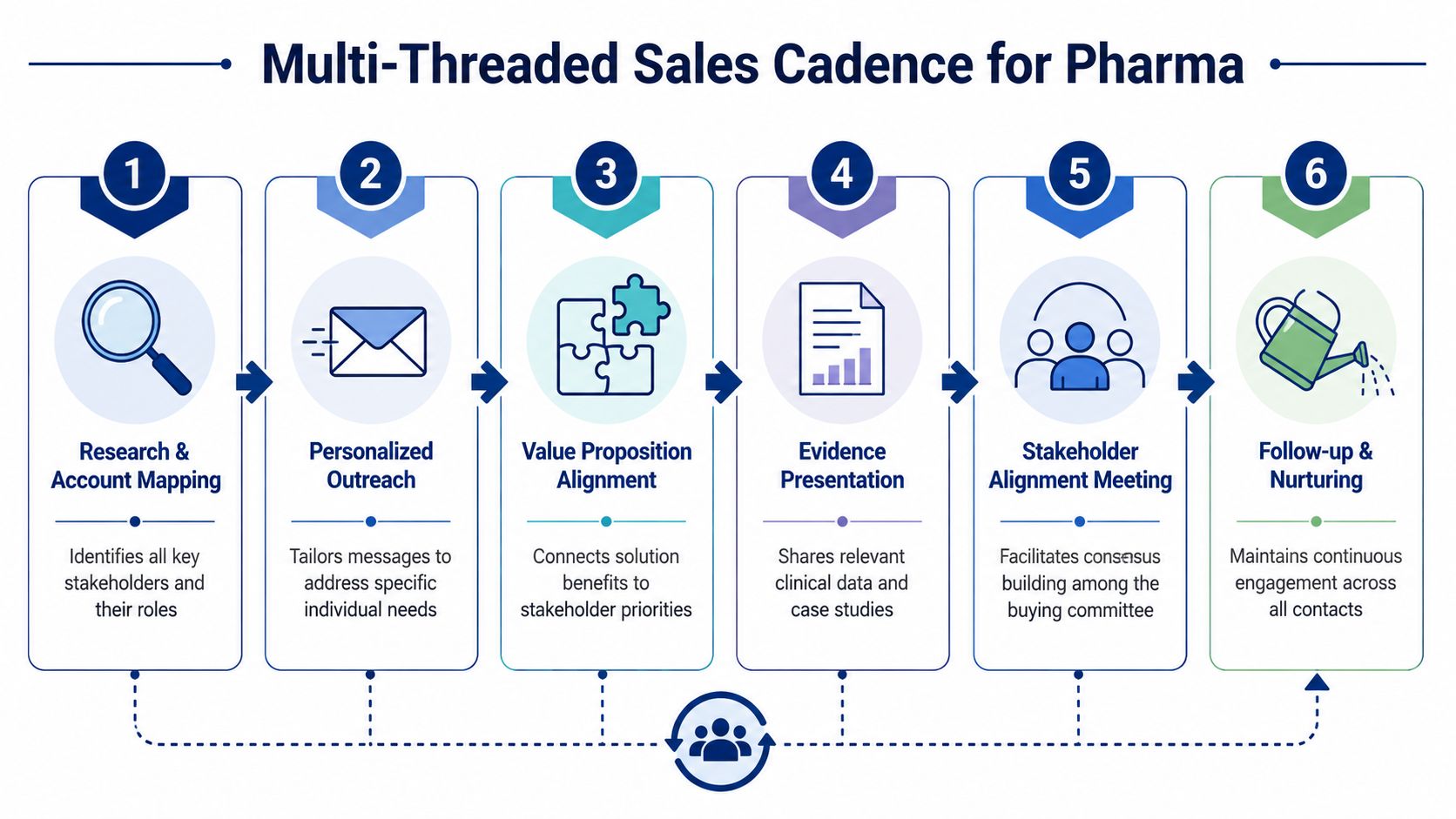
A useful cadence in pharma isn't just multi-channel. It's role-specific and coordinated. Each stakeholder should receive a message tied to the same account thesis, but translated for their priorities.
Here's a practical example over several weeks.
-
Week one, commercial leader
Send an email tied to the trigger event. Focus on launch risk, stakeholder alignment, patient journey friction, or execution readiness. Keep the ask light. -
Week one, clinical or medical stakeholder
Send a separate note referencing the same business moment but from the angle of accuracy, evidence handling, or operational fit. Don't just CC them on the commercial email. -
Week two, IT or data stakeholder
Reach out with a clean note about integration, governance, security review readiness, and implementation scope. This reduces the chance that technical risk becomes a late-stage objection. -
Week two, champion path
Engage the contact most likely to feel the pain first. Share something relevant, short, and usable. A smart question beats a brochure. -
Week three, cross-functional meeting ask
If there's engagement from more than one side, ask for a working session with the right mix of stakeholders. Not a generic demo. A discussion around the account's current initiative.
For teams building this muscle, a practical guide to multi-threading sales strategy can help formalize the approach.
Persona-specific message angles
The message should change by contact. The account thesis shouldn't.
-
Head of Clinical Operations
Focus on workflow fit, evidence quality, review burden, and whether your solution creates or removes process risk. -
VP of Commercial or Commercial Operations
Focus on launch execution, visibility across teams, patient journey friction, and whether decisions are getting stuck between functions. -
Director of IT or IT Procurement
Focus on system fit, data handling, implementation burden, and whether your team is ready for the internal review process.
What not to do in the cadence
A lot of outreach sequences fail because they confuse persistence with relevance.
Avoid these moves:
- Don't send the same email to every stakeholder. They'll compare notes, and it signals you haven't done the work.
- Don't ask for a demo too early. In pharma, the first useful meeting is often about problem definition and stakeholder fit.
- Don't hide procurement topics until late stage. If your compliance posture matters, surface it before the account has to ask.
- Don't over-automate the language. Precision matters more than volume in this vertical.
A strong pharma cadence feels like coordinated account planning in public. Each touchpoint should make the next conversation easier.
That's the standard. If your sequence doesn't build internal consensus, it's probably just creating noise.
Operationalizing Your Pharma Sales Playbook
Pharma teams do not lose deals because the playbook is missing. They lose them because the playbook lives in a slide deck while reps default to generic outreach under pressure.
Execution breaks first.
In this market, discipline matters more than volume. Reps have to track scientific, regulatory, commercial, and organizational change at the account level, then turn that context into outreach a buyer will respect. If that work depends on individual heroics, quality drops fast as the team grows.
The fix is to build an operating model that makes good judgment repeatable.
Build a repeatable operating rhythm
Selling to pharmaceutical companies should run on a weekly review cadence with clear inspection points. The goal is not more meetings. The goal is to keep account hypotheses current and tie outreach to real account movement.
Use account reviews to answer a short list of practical questions:
-
What changed in the account?
Look for leadership changes, clinical milestones, commercial expansion, new partnerships, or signs of budget movement. -
Who now carries influence?
Buying committees shift. One new executive, program lead, or procurement owner can change who needs to be involved early. -
What is our current account thesis?
Every target account needs a specific reason it may act now, based on company context, not a recycled industry pain point. -
What evidence supports the next touch?
Reps should point to observable company activity, then explain why it matters to that stakeholder.
Tooling supports this process, but it does not replace judgment. Teams usually pull from CRM data, company filings, press releases, earnings transcripts, LinkedIn, and industry databases. Salesmotion can fit into that stack as a signal-monitoring tool that helps reps spot changes and prepare outreach with stronger context. The value is consistency. Reps spend less time stitching inputs together by hand and more time deciding where to act.
What sales leaders should inspect
A pharma sales leader who only tracks top-of-funnel activity will get busy teams and weak pipeline quality. Calls and emails are easy to count. Good judgment is harder to inspect, but that is what determines whether an account opens up.
Review process quality instead:
| What to inspect | Why it matters |
|---|---|
| Signal quality | Not every account event merits outreach. Teams need to separate noise from changes that create urgency or internal review. |
| Stakeholder coverage | Deals stall when the rep has one friendly contact and no cross-functional support. |
| Message relevance | Activity without account context produces polite replies at best and silence at worst. |
| Post-trigger speed | Timing decays fast after a visible change in the business. |
| Deal progression after multi-threading | This shows whether the team is building internal alignment or just collecting meetings. |
Listen to call recordings. Read first-touch emails. Check whether the rep connected the signal to a business consequence, then tied that consequence to the right stakeholder's priorities. That is the standard.
Scale judgment, not just activity
Strong pharma organizations turn domain fluency into process. They do not leave it to the few reps who happen to know the industry well.
That usually shows up in a few concrete ways:
- Shared account briefs so every rep starts from the same facts and current account thesis.
- Signal definitions so teams know which changes justify outreach and which ones do not.
- Persona talk tracks so clinical, commercial, IT, and procurement conversations stay distinct.
- Review standards so managers reward timing, specificity, and account understanding instead of raw activity counts.
The aim is simple. Send fewer low-value touches. Create more credible conversations at the moments when the account is most likely to pay attention.
Pharma is relationship-driven, but relationships here are built through informed timing and useful context. Reps earn the next meeting by showing they understand what changed, why it matters, and who inside the account now has to care.