The sites that hit enrollment targets on your last oncology trial are probably the wrong pick for your next rare disease study. And the feasibility questionnaire you sent them will not tell you that.
Clinical trial site selection is treated as an operational problem: check the boxes on investigator qualifications, patient access, and infrastructure, then activate the sites you have used before. But the data tells a different story. According to Tufts CSDD, nearly half of all investigative sites under-enroll or fail to recruit a single patient. Phesi's analysis of cancer trials found that single-patient sites drag down enrollment rates, inflate operational costs, and dilute resources from the sites actually performing. The industry responds by over-selecting sites, which further erodes sponsor-site trust and drives up costs.
The real issue is not site capability. It is the disconnect between what sponsors know about a site's past performance and what actually predicts success on a specific protocol. And for CROs, sites, and service providers trying to win more studies, understanding that disconnect is the difference between getting selected and getting ignored.
TL;DR: Site selection fails because sponsors rely on familiarity and static feasibility data. Performance is protocol-specific, not transferable. Teams that combine predictive analytics (where are the patients?) with signal intelligence (when are sponsors making decisions?) win more studies and build lasting partnerships. The organizations that connect their feasibility data to commercial intelligence have a structural advantage over those that treat them as separate functions.
Your Best Sites Last Year Are Often the Wrong Pick for This Trial
This is the uncomfortable truth that most clinical operations teams avoid confronting: site performance does not transfer reliably across protocols.
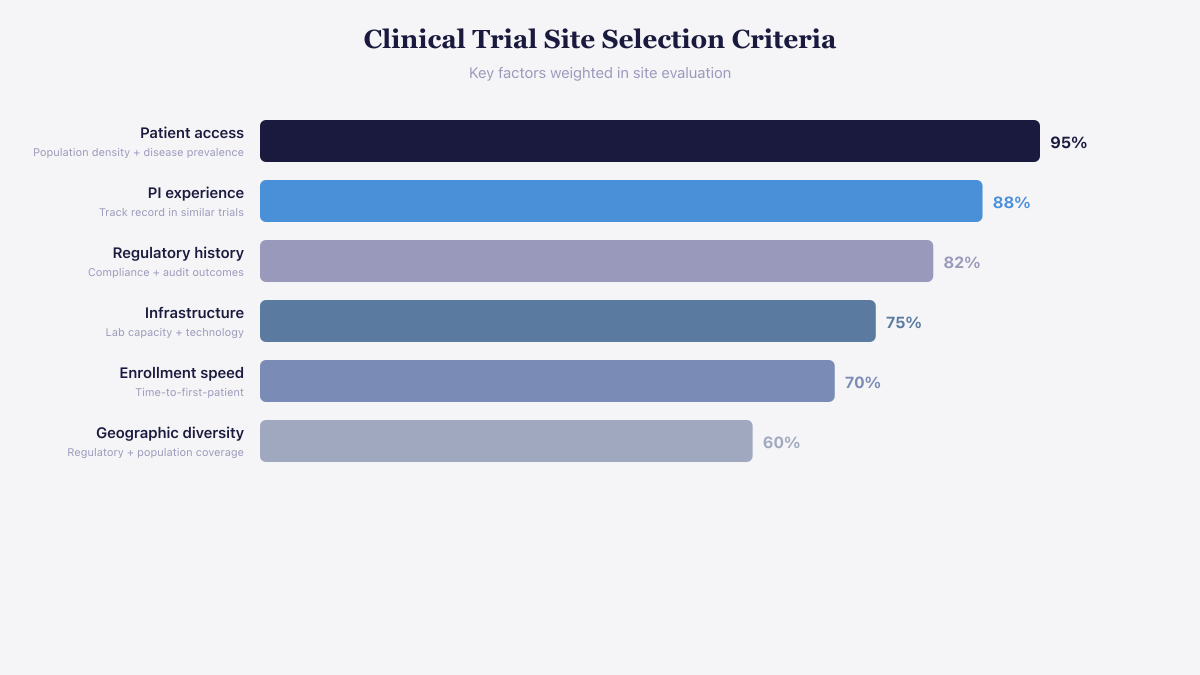 Patient access and principal investigator experience are the highest-weighted site selection factors.
Patient access and principal investigator experience are the highest-weighted site selection factors.
A Circulation: Heart Failure study found that despite uniform selection criteria, patients from sites of varying enrollment volume were "markedly different and at differing risk of trial end points, even after adjustment for conventional risk factors." The researchers attributed this to selection biases across sites, driven by different interpretations of inclusion criteria and varying quality of local recruitment infrastructure.
In practical terms, a site that enrolled 40 patients in a Phase 3 cardiovascular trial might enroll zero in a Phase 2 rare disease study. The PI's therapeutic familiarity changes. The patient catchment area may not overlap with the new indication. The site's experience with specific biomarkers, endpoints, or measurement techniques (increasingly important in precision medicine) may not exist.
Yet sponsors keep defaulting to known networks. Only about 30% of sites in a typical multi-center trial have worked with that specific sponsor before, which sounds like sponsors are casting wide nets. They are not. They are casting the same net in the same water. Meanwhile, 40% of investigators choose not to conduct further trials each year, so the pool itself keeps shifting underneath static selection models.
The contrarian position here is simple: stop treating past enrollment numbers as predictive of future performance. They are descriptive of a different protocol, a different patient population, and often a different competitive landscape for recruitment. What actually predicts success is protocol-specific fit, and assessing that requires intelligence that most feasibility processes never capture.
See Salesmotion on a real account
Book a 15-minute demo and see how your team saves hours on account research.
The Disconnect Between Feasibility Data and Commercial Intelligence
Most CROs and sponsor organizations run two completely separate systems. On the clinical operations side, there is feasibility data: investigator databases, historical enrollment metrics, site qualification visit reports. On the commercial side, there is business development intelligence: which sponsors are funding new programs, which CROs are winning mandates, where the RFPs are flowing.
These systems almost never talk to each other.
The consequence is that commercial teams prospect sponsors without understanding the operational realities of site performance, while clinical operations teams select sites without visibility into the competitive landscape for investigator attention. A site might look perfect on paper, but if that PI is already committed to three competing trials in the same therapeutic area, your enrollment projections are fiction.
This is where account intelligence changes the equation. When you connect sponsor pipeline data, clinical trial registry signals, and commercial relationship intelligence into one view, you can answer questions that neither system addresses alone:
- Which sponsors are actively planning new studies in therapeutic areas where your sites have genuine patient access?
- Which of your investigators are overcommitted, and which have capacity that aligns with upcoming protocols?
- Where are enrollment delays creating rescue opportunities, and can you respond before the sponsor's preferred network fills the gap?
The organizations that connect these systems have a structural advantage. They prospect the right sponsors at the right time, position the right sites for the right protocols, and build a feedback loop between commercial wins and operational performance.

“The AI templates were a surprise delight. We expected the data, but the pre-built email suggestions turned out to be much better than expected and a huge help, especially for newer reps.”
Sabina Malochleb-Bazaud
Senior Sales Operations Administrator, Cytel
What a Signal-to-Selection Sequence Actually Looks Like
Frameworks are useful. Seeing one in action is better. Here is an anonymized walkthrough based on patterns we observe across life sciences commercial teams.
Week 1: The signal fires. A mid-size biotech publishes positive Phase 2 interim results for a NASH therapy. The data appears in a press release on January 15 and is followed by a ClinicalTrials.gov status update indicating the sponsor is planning a Phase 3 expansion with 120 additional sites across North America and Europe.
Week 1-2: Research and alignment. The CRO's business development team pulls the sponsor's pipeline, identifies the VP of Clinical Operations from recent conference presentations, and reviews the sponsor's past trials in metabolic disease. They find that the Phase 2 had enrollment challenges in two geographies, with three sites producing zero patients. They also note the sponsor recently hired a new Head of Site Management, a signal that site network decisions are actively being reassessed.
Week 2: Signal-driven outreach. The BD lead sends a short email referencing the positive Phase 2 results, congratulating the team, and noting that their CRO has site networks with strong hepatology and endocrinology referral relationships in the geographies where Phase 2 under-enrolled. The email proposes a 20-minute call to discuss feasibility alignment, not a generic capabilities presentation.
Week 3: The conversation. The sponsor responds. The call focuses on specific enrollment challenges from Phase 2 and how the CRO's site network addresses them. The CRO shares anonymized enrollment data from comparable protocols, not just general capabilities.
Week 6: Shortlisted. The CRO is included in the RFP for Phase 3 site management. They entered the process two months before the RFP was published because they acted on the signal when it appeared.
This is the difference between reactive prospecting (waiting for the RFP) and proactive intelligence (engaging during the decision window). According to recent industry data, trigger-based outreach like this drives response rates of 15 to 25%, compared to 1 to 2% for generic cold emails. For a deeper look at these buying signals in practice, see our guide to signal-based prospecting in life sciences.
Where Predictive Analytics Falls Short (and What Fills the Gap)
The industry is investing heavily in predictive site selection, and for good reason. The AI-powered clinical trial site feasibility market hit $1.53 billion in 2025 and is projected to reach $3.55 billion by 2029. Machine learning models from organizations like Janssen are outperforming traditional methods at ranking sites by expected recruitment, using EHR data, claims data, and geo-demographic modeling.
These tools answer a critical question: where are the patients? EHR-based feasibility can model real patient counts, comorbidities, medication patterns, and visit frequency with far more accuracy than a feasibility questionnaire filled out by an optimistic site coordinator. Geo-demographic modeling helps sponsors meet the FDA's new Diversity Action Plan requirements, which became binding in late 2025, by identifying sites with access to underrepresented populations.
But predictive analytics has a blind spot. It tells you where patients are. It does not tell you when sponsors need them.
A site might have the ideal patient population for a rare disease protocol, but if no sponsor is actively planning a trial in that indication, the intelligence is inert. Conversely, when a sponsor posts positive Phase 2 results and begins site selection for Phase 3, the window to engage is weeks, not months. Predictive patient data without commercial timing intelligence is a catalog without a buyer.
The teams winning the most studies combine both: predictive analytics to identify protocol-specific site fit, and signal intelligence to engage sponsors during the decision window. Neither is sufficient alone.

“All of the vendors that I've worked with, all of the onboarding that I have had to deal with, I will say, hands down, Salesmotion was the easiest that I have had.”
Lyndsay Thomson
Head of Sales Operations, Cytel
The Sponsor Side: Managing Site Networks with Intelligence
This article would be incomplete if it only addressed how to sell to sponsors. The same intelligence framework applies to sponsor-side teams and large CROs managing existing site networks.
For a Parexel or IQVIA, the challenge is not finding sites. It is managing a network of thousands of sites across geographies and therapeutic areas, and knowing which sites to activate for a specific protocol. Historical performance data helps, but as discussed above, past performance is protocol-specific.
Sponsor-side teams are increasingly using real-time intelligence to:
- Monitor investigator availability and competing commitments. If a high-performing PI just committed to two competing trials, activating that site for your study is a predictable enrollment failure.
- Track regulatory and compliance signals. FDA warning letters, inspection findings, and IRB issues at sites in your network represent risks that static databases do not capture.
- Identify emerging sites before they appear in industry databases. New research programs at academic medical centers, recently credentialed PIs, and sites expanding into new therapeutic areas represent untapped capacity.
The common thread is the same: static data (feasibility questionnaires, investigator databases) provides a snapshot. Intelligence (signals, competitive monitoring, real-time tracking) provides a motion picture. The organizations making the best site selection decisions are watching the motion picture.
What Happens When You Connect the Systems
When Cytel, a global leader in advanced analytics for life sciences, evaluated their commercial workflow, the problem was structural. Their team toggled across five or more disconnected tools to prepare for a single sponsor conversation. Inside sales reps spent hours on manual account research before they could even assess whether an opportunity was worth pursuing.
The numbers after consolidating into a single intelligence platform:
- Research time cut by 50% across the sales team, freeing dozens of selling hours per rep per quarter
- Account planning prep reduced by 30%, directly accelerating QBR and pipeline review cycles
- Five disconnected tools replaced by one, eliminating context-switching and ensuring consistent intelligence across team members
- New hire ramp time compressed through AI-generated messaging templates that doubled as a learning tool for understanding accounts, therapeutic areas, and sponsor priorities
Jillian Cormier, VP of Business Development at Cytel, described the shift: for newer reps, the platform functions as both a research tool and a learning tool, helping them understand the account, the context, and how to message effectively without needing weeks of training.
The operational impact is measurable. If each account conversation requires two to three hours of manual research (the pre-automation industry average), a team of ten reps loses 100 to 150 hours per month to research alone. Cutting that in half returns over a thousand selling hours per year, and those hours go directly into sponsor conversations, not database browsing.
Key Takeaways
- Past site performance does not reliably predict future enrollment. Performance is protocol-specific. Stop treating historical enrollment numbers as the primary selection criterion.
- Most organizations waste their feasibility data by never connecting it to commercial intelligence. Bridging clinical operations data with business development signals creates a structural advantage.
- Predictive analytics tells you where patients are. Signal intelligence tells you when sponsors need them. You need both, and neither is sufficient alone.
- Trigger-based outreach generates 15 to 25% response rates, compared to 1 to 2% for generic emails. The difference is acting during the decision window, not after it closes.
- The FDA's Diversity Action Plan requirements (binding since late 2025) are reshaping site selection. Geo-demographic modeling is no longer optional.
- Consolidating intelligence into one system delivers measurable results. Cytel cut research time by 50% and account planning prep by 30% across their commercial team.
Frequently Asked Questions
Why do so many clinical trial sites fail to enroll patients?
Site enrollment failure is protocol-specific, not a reflection of general site capability. A site that performs well in one therapeutic area may lack the patient population, investigator expertise, or endpoint measurement experience for a different protocol. According to Tufts CSDD, 37% of sites under-enroll and 11% fail to enroll a single patient. The root causes include overly optimistic feasibility assessments, investigator overcommitment to competing trials, and a disconnect between sponsor site selection criteria and actual protocol requirements.
How are FDA diversity requirements changing clinical trial site selection?
The FDA's Diversity Action Plans, mandated under FDORA and binding since late 2025, require sponsors to submit enrollment targets disaggregated by race, ethnicity, sex, and age group. This means site selection must now account for the demographic composition of a site's patient population, not just its enrollment history. Sponsors are using geo-demographic modeling and EHR data to identify sites with access to underrepresented populations, and sites that can demonstrate diverse patient access have a growing competitive advantage.
What is the difference between predictive site selection and signal-based prospecting?
Predictive site selection uses historical data, EHR records, and machine learning to estimate which sites are most likely to enroll patients for a specific protocol. It answers "where are the patients?" Signal-based prospecting monitors sponsor activity, including buying signals like funding rounds, phase transitions, enrollment delays, and leadership changes, to identify when sponsors are actively making site selection decisions. The most effective teams combine both approaches: predictive analytics for protocol-specific fit and signal intelligence for commercial timing.
How long does it typically take from signal identification to site selection?
The timeline varies by sponsor size and trial complexity, but the window between a signal (such as positive Phase 2 results) and the start of formal site selection is typically four to eight weeks. From initial site identification to first patient enrollment, the full process averages around eight months. Teams that engage during the early signal window, before the RFP is published, have significantly higher success rates than those who enter the process reactively.


