CRO stocks have fallen off a cliff. IQVIA, Medpace, and Charles River Laboratories all dropped sharply after Anthropic launched advanced AI agents in February, and investors started asking whether drugmakers could just bring clinical trial work in-house. The market erased $7.3 billion from IQVIA's market cap alone, despite strong Q4 results. A wave of pharma-AI partnerships added fuel. The narrative hardened fast: AI will eat CROs.
The narrative is wrong. But not for the reasons most people think.
TL;DR: Wall Street panicked about AI replacing CROs. The operational backbone of clinical trials cannot be automated away. But the market is right that AI reshapes CRO economics, it is just wrong about where. The CROs that win the next decade will not be the ones running trials marginally faster. They will be the ones engaging sponsors 6-9 months earlier, during protocol planning rather than at RFP, and converting that early positioning into higher win rates and preferred provider status. That is a commercial intelligence problem, and AI is solving it now.
The Selloff: What Happened and Why It's Overblown
Reuters reported in late March that shares of major CROs have tumbled on fears that AI advances could allow drugmakers to take clinical trial work in-house. The concern is straightforward: if AI can handle protocol design, patient matching, and data analysis, why pay a CRO to do it?
Industry experts pushed back hard. Jailendra Singh, analyst at Truist Securities, noted that CROs maintain global networks of trial sites and hold proprietary data that pharma companies, especially smaller biotechs, cannot easily replicate. TD Cowen estimated that even a fully AI-enabled clinical trial setup would deliver only 10-15% cost savings for drugmakers. That is notable, but not existential for a $100 billion industry growing at nearly 9% annually. The savings range also varies enormously by therapeutic area and trial complexity, which is something Wall Street models tend to flatten.
Ami Bhatt, chairperson of the U.S. FDA's Digital Health Advisory Committee, made the regulatory case clearly: AI could automate high-volume tasks such as patient pre-screening, but critical decisions still require human oversight. Site execution, informed consent, and safety monitoring remain firmly in human hands, with accountability ultimately resting on people.
Truist's Singh was blunt about the selloff: "We do not see AI as a headwind for the industry; if anything, it is more of a tailwind." There is no evidence of pharma companies cutting spending with CROs because of AI.
Where AI Actually Changes CRO Economics
Christian Hein, a health AI builder scaling AI in biopharma, put it sharply on LinkedIn: "The market may be right that AI changes the economics of trials. It is wrong about where the disruption lands."
His argument deserves attention. TD Cowen estimates AI could compress a late-stage trial from 58 months to 47. That is real. Protocol design, site selection, data monitoring, signal detection: AI will reshape all of these. But the hardest part of running a clinical trial is the operational complexity that no model can replicate. Patient recruitment across 200 sites in 40 countries. Navigating regulatory submissions in jurisdictions with different safety reporting timelines. The 2 AM call when a site in Brazil loses its principal investigator mid-enrollment. Maintaining GCP compliance across a decentralized trial with 15 different electronic data capture systems.
CROs are infrastructure companies that Wall Street keeps pricing like software vendors.
And the real irony, as Hein points out: AI should make CROs more valuable, not less. The firms that integrate AI into trial execution will compress timelines and capture the upside. TD Cowen already sees new contracting models emerging, including gain-share arrangements where CROs keep a portion of the time savings they deliver. For a drug with estimated peak annual revenues of $1.5 billion, reaching the market nearly a year earlier could mean tens of millions in additional revenue, the exact economics depend heavily on the therapeutic area, competitive landscape, and payer dynamics, but the directional incentive is enormous.
The question worth asking is not whether AI will replace CROs. It is which CRO will be first to price its contracts based on AI-enabled speed.

“Salesmotion is helping Cytel elevate our enterprise sales performance by embedding account intelligence directly into our workflow. The platform gives our commercial team real-time visibility into key account movements.”
Jonathan Burr
Chief Commercial Officer, Cytel
The 11 Months Start Before the Trial Does
Here is where most analysis of AI in CROs stops. Trial execution gets faster. Enrollment improves. Data monitoring becomes more efficient. That is all true, and it matters.
But the 11-month compression that TD Cowen models does not begin when the first patient is enrolled. It begins when the CRO first engages the sponsor.
Any CCO at a top-20 CRO knows this: the biggest determinant of whether you win a program is not your bid price or your site network. It is when you enter the conversation. CROs that engage sponsors during protocol planning, before the RFP is written, shape the trial design itself. They influence site selection criteria, enrollment strategy, and operational scope. By the time a formal RFP goes out, the CRO that helped shape it has a structural advantage that late entrants cannot overcome with a better proposal.
This is the pattern that played out across the industry in the last cycle of mega-trials. IQVIA's preferred provider agreements with top-20 pharma sponsors did not come from responding faster to RFPs. They came from embedding commercial and scientific teams early enough to influence the program strategy. ICON plc built similar positions through strategic consulting relationships that preceded formal outsourcing decisions. Medpace carved out a mid-cap niche by developing deep therapeutic expertise that sponsors brought in during protocol feasibility, not procurement.
The common thread: early engagement wins programs. Late engagement competes on price.
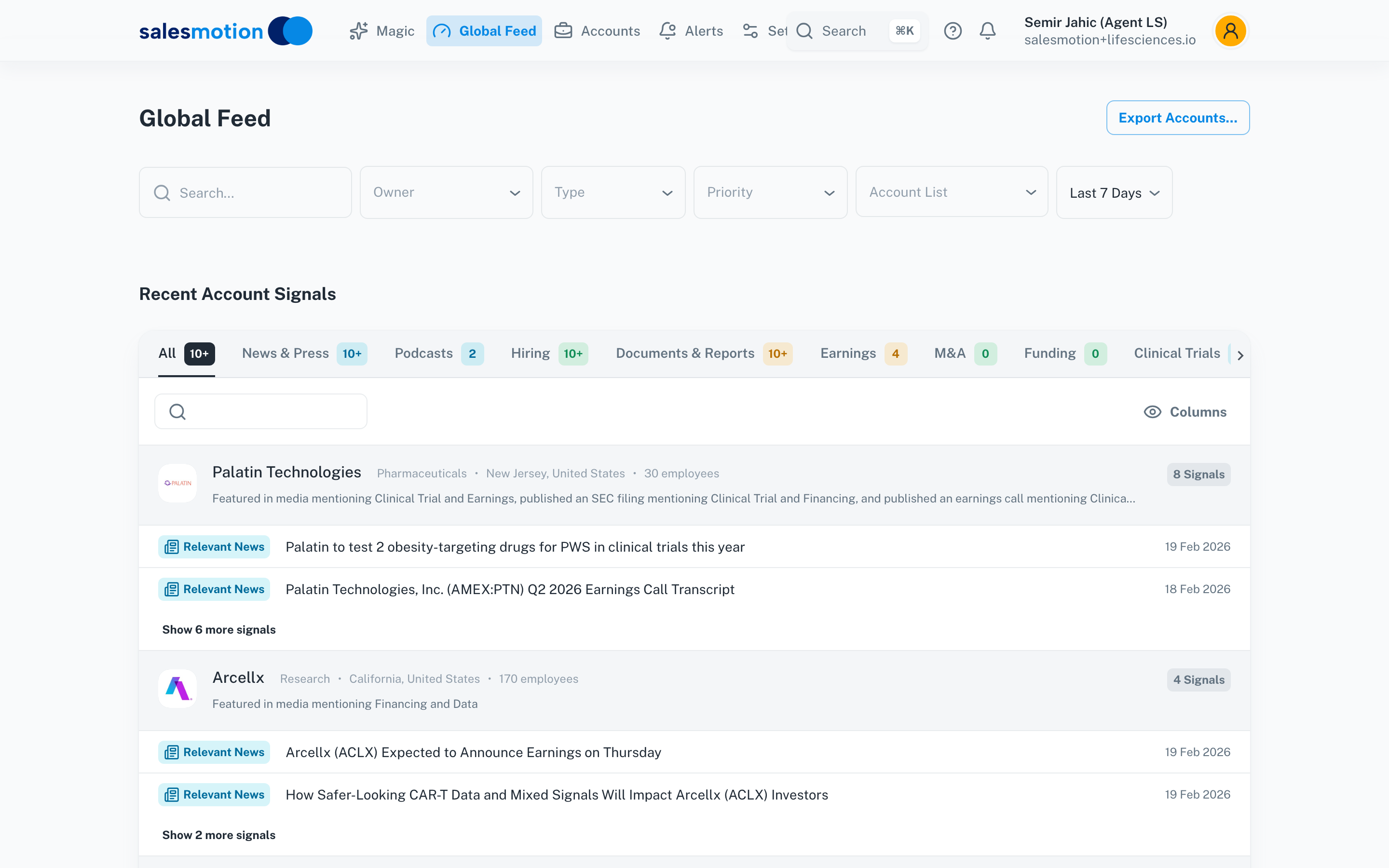
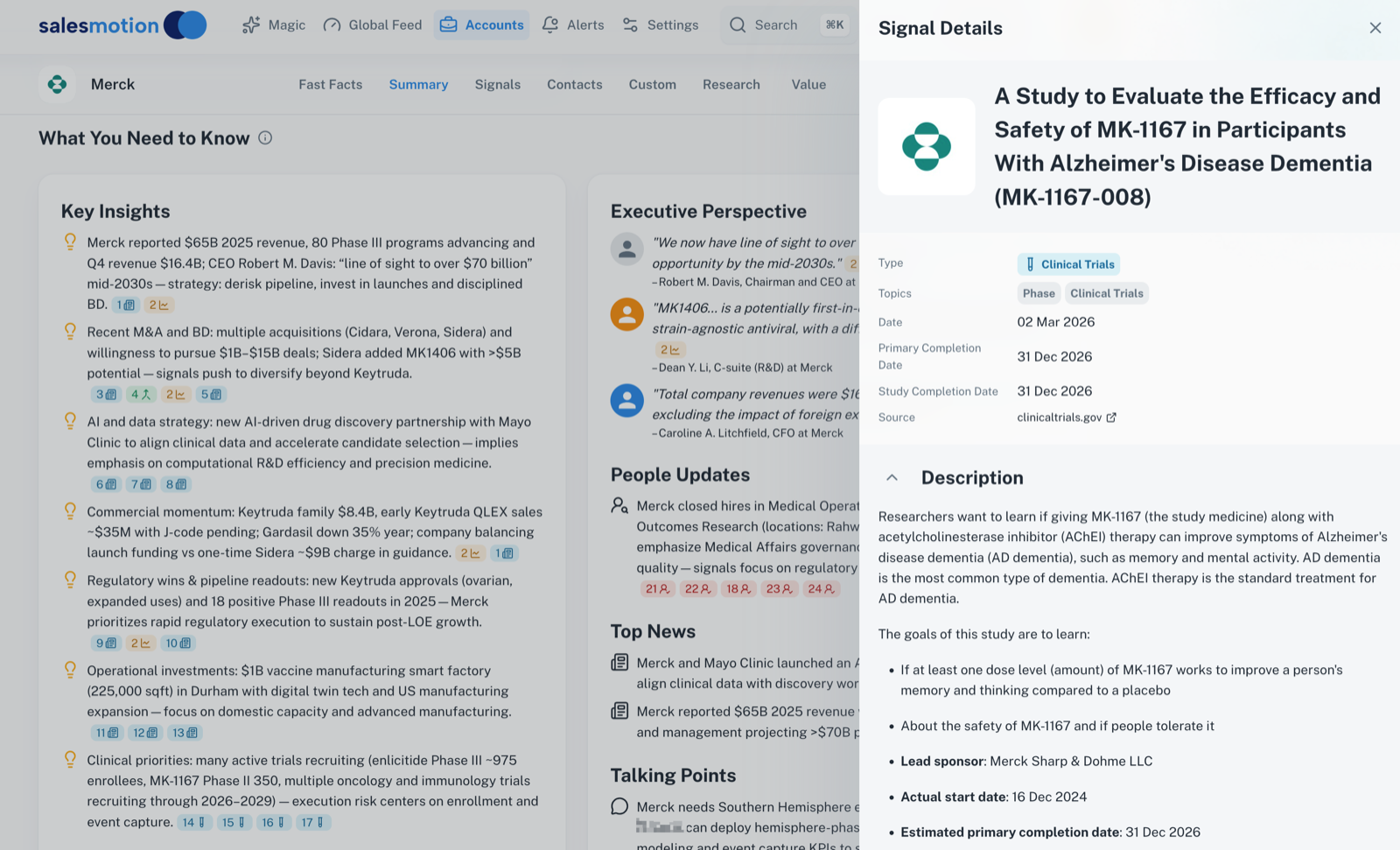 Clinical trial intelligence for a pharma account, showing pipeline activity, trial phases, and enrollment signals in one view.
Clinical trial intelligence for a pharma account, showing pipeline activity, trial phases, and enrollment signals in one view.
This is where AI transforms the competitive dynamics for CROs, not by making trials faster, but by making the commercial engine faster. If your BD team identifies a sponsor's Phase III readiness signal six months before your competitor does, you engage during protocol planning while they respond to the RFP. You shape the trial. They bid on it.
The signals are visible to anyone paying attention: hiring surges in clinical operations roles, patent filings in new therapeutic areas, earnings call language about "pipeline acceleration," and executive hires that signal commercial readiness. These leading indicators surface 3-6 months before a trial hits ClinicalTrials.gov. The question is whether your commercial team is set up to capture them systematically, or still relying on relationship networks and quarterly pipeline reviews.
What This Looks Like in Practice
Cytel offers a useful case study. As a clinical research analytics firm with 2,000+ employees and $329 million in revenue, Cytel sits at the intersection of biostatistics, adaptive trial design, and regulatory strategy. Their software, including East and the East Horizon platform, is used by the FDA, the EMA, and the world's top 30 biopharma companies.
Cytel's commercial challenge was not a lack of relationships. It was timing. Their BD team was tracking sponsor pipelines across five separate systems: ZoomInfo for contacts, Crunchbase for funding signals, SEC filings for strategic direction, Google News for announcements, and ClinicalTrials.gov for program activity. By the time those signals were manually synthesized into an actionable view, competing CROs had already engaged the sponsor.
They consolidated into a single account intelligence platform and saw 50% reduction in research time and 30% faster account planning. But the number that matters most is harder to measure directly: earlier engagement. When your BD team can identify a sponsor's pipeline expansion in real time, cross-referenced with hiring patterns and earnings commentary, the conversation starts during planning rather than procurement. Jonathan Burr, Cytel's Chief Commercial Officer, framed the impact as elevating "enterprise sales performance," not just saving time, but fundamentally changing when and how they engage key accounts.
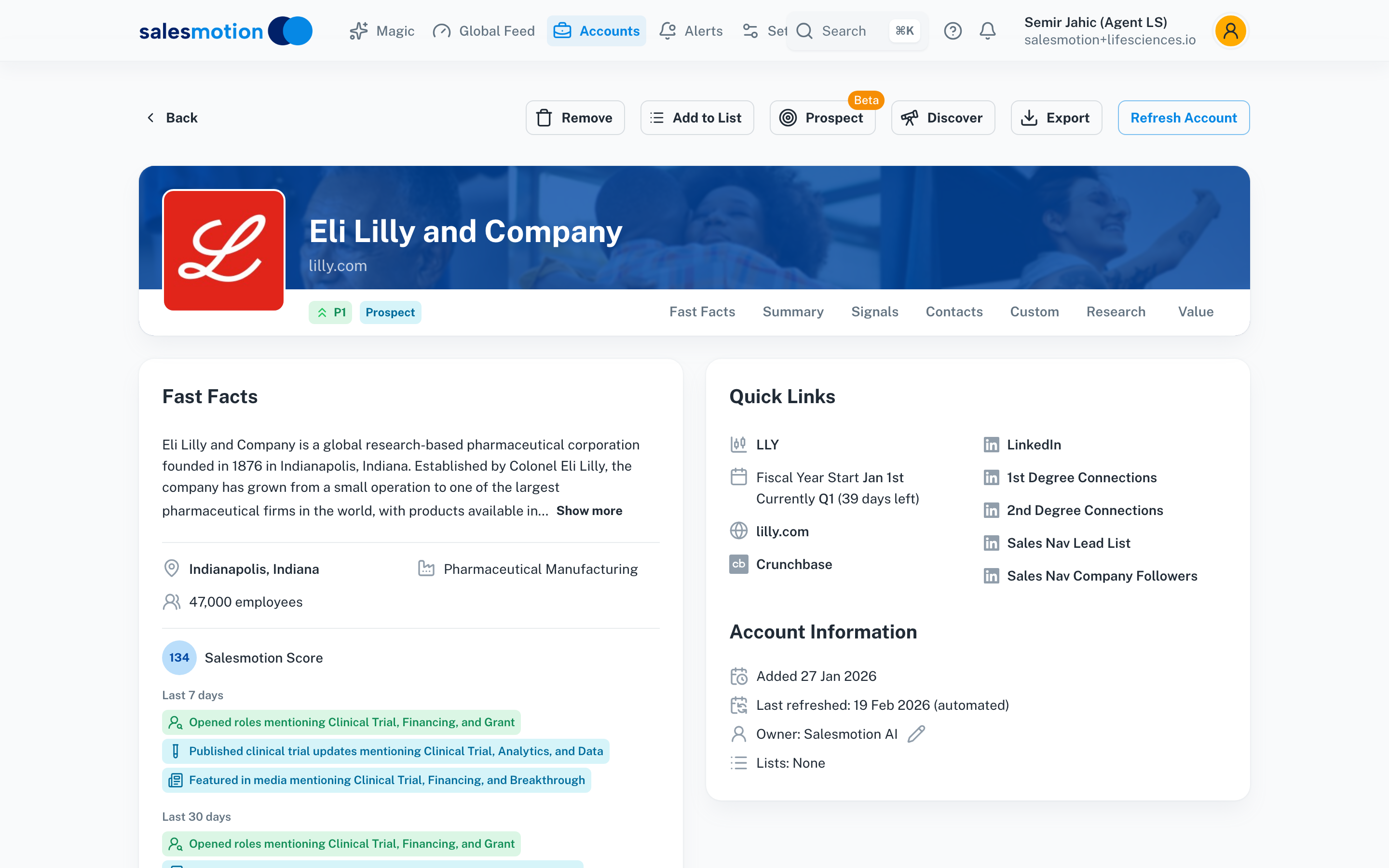 An account summary for a life sciences prospect, consolidating clinical pipeline data, strategic initiatives, and competitive signals into one research view.
An account summary for a life sciences prospect, consolidating clinical pipeline data, strategic initiatives, and competitive signals into one research view.
That distinction matters because the economics of CRO business development are nonlinear. Engaging a sponsor during protocol design does not just improve your odds marginally. It changes the nature of the relationship from vendor to strategic partner. And strategic partners get preferred provider agreements, which drive multi-year revenue predictability, the metric every CRO CCO is measured on.
See Salesmotion on a real account
Book a 15-minute demo and see how your team saves hours on account research.
The Competitive Map Is Shifting
The CRO market is not monolithic, and AI will not affect every player equally.
IQVIA has the deepest data assets in the industry, including Real World Data from 1.2 billion patient records and a massive clinical trial database. They are best positioned to embed AI into trial design and site selection. But their size also creates inertia. IQVIA recently acquired portions of Charles River's discovery business for $145 million, signaling a bet on upstream integration rather than AI-driven commercial transformation.
Medpace has built a strong position in mid-cap biotech by offering deep therapeutic expertise and operational discipline. Their value proposition is less vulnerable to AI disruption because it rests on scientific judgment, not data processing. But they face a challenge: if larger CROs use AI to move faster in the same therapeutic areas, Medpace's expertise advantage narrows.
Mid-tier and specialty CROs face the most acute pressure. They lack the data scale of IQVIA and the therapeutic depth of Medpace. For these firms, AI-driven commercial intelligence is not optional. It is the most direct path to competing for programs that would otherwise go to larger incumbents. The CROs in this tier that equip their BD teams with real-time signal monitoring and automated sponsor intelligence will punch above their weight. Those that do not will find themselves perpetually responding to RFPs they had no hand in shaping.
A sharp divide is forming between organizations building AI fluency into every layer of their operations and legacy operators still piloting standalone use cases. That divide is visible in clinical operations. It is equally visible, and arguably more consequential in the short term, in commercial operations.
The Gain-Share Inflection Point
The cost-plus model has served CROs well for decades. As Hein noted, it will be painful to give up. The current inertia is real: "nobody ever got fired for hiring IBM." If the future of your large Phase III trial depends on your head of clinical operations delivering, the safe choice is the approach that has worked for decades.
But TD Cowen sees the model shifting. Gain-share arrangements, where CROs keep a portion of the time savings they deliver, fundamentally change incentives. Under cost-plus, there is no reward for efficiency. Under gain-share, the CRO that brings a trial in 47 months instead of 58 captures direct financial upside.
This creates a compounding advantage. CROs that invest in AI, both in trial execution and commercial operations, deliver faster timelines. Faster timelines unlock gain-share revenue. That revenue funds further AI investment. The flywheel favors early movers.
 Real-time signal monitoring across life sciences accounts, surfacing earnings events, leadership changes, and competitive moves as they happen.
Real-time signal monitoring across life sciences accounts, surfacing earnings events, leadership changes, and competitive moves as they happen.
For CRO commercial leaders, this is the strategic question: are you investing in the commercial intelligence infrastructure that positions you for gain-share contracting? Or are you waiting for sponsors to demand it?
Key Takeaways
- CRO stock selloffs are overblown. There is no evidence of pharma companies cutting CRO spending because of AI. The operational backbone of clinical trials, patient recruitment, regulatory compliance, site management, cannot be automated away.
- The 11-month compression starts before the trial. AI-enabled CROs win by engaging sponsors during protocol planning, not at RFP. Early engagement shapes trial design and converts to preferred provider status.
- Commercial speed is the overlooked advantage. CROs that identify sponsor pipeline signals 6-9 months earlier win more Phase II-III programs. That is a commercial intelligence problem, not a clinical execution problem.
- The competitive map favors AI fluency. IQVIA has data depth, Medpace has therapeutic expertise, but mid-tier CROs that deploy AI-driven commercial intelligence can compete for programs above their traditional weight class.
- Gain-share contracting rewards AI investment. New models where CROs capture time-savings upside create a flywheel: faster timelines fund further AI investment, which drives faster timelines.
- The cost-plus model will not protect incumbents indefinitely. CROs building AI fluency across clinical and commercial operations are pulling ahead. Those still running isolated pilots will fall behind.
Frequently Asked Questions
Will AI replace contract research organizations?
No. Industry analysts and executives are clear that AI cannot replace the operational backbone of clinical trials. Patient recruitment across hundreds of sites, regulatory compliance across jurisdictions, informed consent, and safety monitoring all require human oversight and accountability. TD Cowen estimates only 10-15% cost savings from fully AI-enabled trials, though the actual range varies significantly by therapeutic area and trial complexity. The FDA's Digital Health Advisory Committee chair has emphasized that critical clinical decisions remain firmly in human hands.
How does AI change CRO competitive dynamics?
The most significant impact is on timing. CROs that use AI to identify sponsor pipeline signals, hiring surges, patent filings, earnings commentary, regulatory milestones, can engage sponsors during protocol planning rather than at RFP. This early engagement converts to higher win rates and preferred provider agreements. The effect is most pronounced for mid-tier CROs competing against IQVIA and ICON, where commercial speed can offset scale disadvantages.
What are gain-share arrangements in CRO contracting?
TD Cowen identifies gain-share contracts as an emerging model where CROs keep a portion of the time savings they deliver through AI-enabled efficiency. Instead of billing cost-plus, the CRO shares in the financial upside of faster trial completion. For a drug with estimated peak annual revenues of $1.5 billion, even modest timeline compression creates significant value. This model rewards CROs that invest in AI and penalizes those that rely on traditional cost-plus billing.
Which CROs are most at risk from the AI shift?
The CROs most at risk are not facing replacement by AI, but competitive displacement by peers that adopt it faster. Mid-tier CROs without deep data assets (like IQVIA's) or therapeutic specialization (like Medpace's) face the most pressure. Those that equip their BD teams with automated signal monitoring and sponsor intelligence will compete effectively for larger programs. Those that continue relying on manual pipeline tracking and relationship-based selling will find themselves responding to RFPs shaped by competitors who engaged months earlier.